Authors: S Soni, S K Pippal, Yashveer B, P Srivastava
Institution: Department of ENT, Gandhi Medical College, Bhopal, India
Corresponding Author:
Dr Smita Soni
Assistant Professor in ENT
GMC, Bhopal
Abstract:
Fine needle aspiration cytology (FNAC) is a simple, quick, inexpensive and minimally invasive technique used to diagnose different types of masses. In otolaryngology, FNAC's greatest utility is in the diagnosis of neck masses. Masses located in the head and neck most commonly originate from cervical lymph nodes, thyroid, parotid and salivary glands.
Purpose: To assess the sensitivity and specificity of FNAC in the diagnosis of neck masses.
Method: A retrospective study was conducted between January 2009 to December 2009. Patient data was collected and details of their neck mass and clinical diagnosis were recorded. FNAC findings suggestive of various pathologies were recorded. Patients between the ages of 5 to 70 years were admitted into the study. A total of 68 patients with a neck lump underwent FNAC.
Results: Out of our total patients, 9 cases had a FNAC that was either acellular or hemorrhagic. These patients were excluded from data analysis. The remaining 59 patients were included in the study. The results of the FNAC were compared with the tissue diagnosis obtained after surgical removal of the mass. Out of 59 patients, in 44 cases the histopathological report confirmed the FNAC diagnosis. In 15 cases, the histopathology report was different.
Out of the 59 fine needle aspiration procedures, 28 (47.45%) were of neck node, 14 (23.72%) were of thyroid, 13 (22.03%) were of salivary gland and 4 (6.77%) were of other neck masses. The overall sensitivity of FNAC in the diagnosis of neck masses was 83.01% and specificity was 78.94%. Sensitivity was highest (82.14%) for neck nodes and lowest for thyroid masses (64.28%). Specificity was the highest for other neck masses (100%) and the lowest for neck nodes (71.2%).
Conclusion: it is concluded that neck masses are very common conditions encountered by an otolarymgologist in his day-to-day practice. Our study found that FNAC is a simple, quick and inexpensive technique to diagnose different types of neck masses. However, its accuracy could have been increased if performed under ultrasound guidance.
Introduction:
The evaluation of a neck mass is a common clinical dilemma and a condition to which an ENT clinician routinely encounters. Commonly presenting neck masses occur within lymph nodes, thyroid, parotid and other salivary glands. Less common pathologies presenting as neck swellings are from thyroglossal cysts, branchial cleft cysts, carotid body tumors, cystic hygromas, pharyngeal pouch abnormalities and lumps of skin appendages.1 Fine needle aspiration cytology (FNAC) is a simple, quick and cost effective method to sample superficial masses found in the neck. The technique is performed in the outpatient clinic. It causes minimal trauma to the patient and carries virtually no risk of complication. Masses located within the region of head and neck including salivary glands and thyroid masses can be readily diagnosed using this technique.2,3 In the head and neck region, FNAC is of great value because of the multiplicity of accessible organs and heterogeneous pathologies encountered. An early differentiation of benign from malignant pathology greatly influences the planned treatment.4 Fine needle aspiration cytology can be performed under local anesthesia and is particularly useful if a neck lump is thought to be malignant. There is no evidence that the tumor spreads through the skin track created by the fine hypodermic needle used in this technique.5 FNAC can be both diagnostic and therapeutic in cystic swellings.6
Fine needle aspiration cytology is helpful for the diagnosis of salivary gland tumor where it can differentiate between a benign and malignant tumor with 90% accuracy.7 FNAC is particularly helpful in the workup of cervical masses and nodules because biopsy of cervical adenopathy should be avoided until all diagnostic modalities have failed to establish diagnosis.8 FNAC is clearly no substitute for histology, especially in determination of nodal architecture in lymphoma, the malignant pattern of follicular thyroid tumor, intracapsular spread in squamous carcinoma or in the distinction of pleomorphic from monomorphic adenoma.4
The purpose of this study was to evaluate the adequacy and accuracy of FNAC in diagnosis of neck mass.
Methods:
This retrospective study was carried out in the Department of ENT, Gandhi Medical College, Bhopal, from January 2009 to December 2009. A total 68 patients with a neck lump underwent FNAC.
Exclusion criteria:
1. Patient who underwent FNAC but did not undergo subsequent histopathological diagnosis.
2. Patients in whom FNAC was either acellular or nondiagnostic.
Inclusion criteria:
1. All the patients of both sexes who presented with a neck lump.
Out of 68 patients, in 9 patients FNAC was either acellular or nondiagnostic, so they were excluded from the study. Out of 59 patients, 39 were female and 20 were male. The youngest patient was a 5 year old and the oldest was a 70 year old. Clinical and FNAC details suggestive of various pathologies were noted. In addition, subsequent histopathology/biopsy details were noted and comparison of histology diagnosis with that of FNAC were made.
Fine needle aspiration cytology (FNAC) was performed without ultrasound guidance by different technicians. A minimum of three passes of the needle were performed on each lesion.
Results
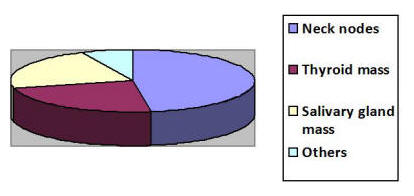
This retrospective study included 59 patients between the ages of 5 to 70 years. 39 patients (66.15%) were females and 20 (33.89%) were males. In 44 patients, out of the 59, subsequent histopathology confirmed FNAC diagnosis (sensitivity 83.01%) and in 15 cases HPR did not confirm FNAC diagnosis (specificity 78.94%). Out of the 59 patients, 28 (47.45%) were of neck nodes, 14 (23.72%) were of thyroid, 13 (22.03%) were of salivary gland masses and 4 (6.77%) were from other types of neck masses (See Figure 1).
Figure 1: Type of Neck Masses Studied
For neck nodes sensitivity of FNAC was 82.14% and specificity was 71.2%. For thyroid masses sensitivity was 64.28% and specificity was 83.3%. For salivary gland masses sensitivity was 67.8% and specificity was 80%. For other neck masses sensitivity was 75% and specificity was 100% (See Figure 2).
Figure 2: Sensitivity and Specificity of Needle Biopsy in Various Types of Neck Masses.

Discussion:
This retrospective study was conducted to determine the sensitivity and specificity of FNAC in the diagnosis of neck masses. The results were then compared with other reports.
Our study evaluated 59 patients and found the overall sensitivity of FNAC in the diagnosis of neck masses to be 83.01% and specificity to be 78.94%. The sensitivity for neck nodes was 82.14% and specificity was 71.2%; for thyroid masses sensitivity was 64.28% and specificity was 83.3%; for salivary gland masses sensitivity was 67.8% and specificity was 80%.
Howlett, D.C., et al., studied a total of 276 patients and found FNAC of neck nodes to have a sensitivity of 89% and a specificity of 57%; for thyroid masses, the sensitivity was 62% and specificity was 86%; and for salivary glands, the sensitivity was 64% and specificity was 100%.
In Hamilton, et al., studied a total of 500 patients with an overall accuracy in diagnosis of 95%.
Tilak, V., Dhaded, A.V., et al., studied 550 patients and found the overall sensitivity of FNAC for neck masses to be 90.91% and specificity to be 93.18% which is greater than that observed in our study. In our study, FNAC was most accurate in the diagnosis of neck nodes (sensitivity 82.14% and specificity 71.2%). However in the Howlett, D.C., et al., study, the sensitivity was 89% and the specificity was 57%. In our study, the sensitivity for the thyroid group was 64.28% and the specificity was 83.3% which was similar to Howlett, D.C., et al.'s results in which sensitivity and specificity were 62% and 86%, respectively. In our study, the sensitivity for the salivary gland group was 67.8% and the specificity was 80%. Howlett, D.C., et al., found a similar sensitivity (64%) but s higher specificity (100%).
Difference in the specificity of the neck node and salivary gland group between our study and Howlett, D.C., et al,. maybe due to differences in the method of aspiration of the neck lump. In our study, blind FNAC was performed by different technicians without ultrasound guidance. In Howlett, D.C., et al., study, ultrasound guided FNAC was used in 50% of the thyroid group and a few parotid patients. The differences might also be explained by differences in the patient population. In India, most patients are illiterate and unaware of their health problems until they are at an advanced stage. The majority of patients present with a huge neck mass which is obvious and easy for the cytopathologist to locate with FNAC without the use of ultrasound guidance. In addition, in such large lesions there may well be a sampling error within the mass itself with different regions of the mass having different grades of pathology.
Another study was reported by Richard Schwarz, et al., in which the authors evaluated 165 patients. In their study, the sensitivity of FNAC for metastatic carcinoma was 92% and for lymphoma was 100%. In their study, the accuracy was highest for the malignant salivary group and lowest for the benign salivary gland group.
Finally, James Edward M., et al, observed an overall accuracy for FNAC of 94.5%. Thyroid metastasis or benign node lesion had an accuracy of approximately 95%. The diagnosis of lymphomatous lesion had a lower accuracy of 75%. In our present study, the accuracy for diagnosis of metastatic neck nodes was approximately 90%, followed by the diagnosis of lymphoma which was 80% and for tubercular lymphadenitis which was 60%. The thyroid group had an accuracy of almost 70%; the benign salivary gland group had an accuracy of 90%; and the overall diagnosis of malignant lesions was 70%.
Table I:

Conclusion:
We can conclude from the present study that FNAC is a simple, rapid, inexpensive and well tolerated procedure for the diagnosis of head and neck masses. It is the most accurate where there is a close cooperation between clinician, cytopathologist and radiologist. Ultrasound guided FNAC allows samples to be taken from a more representative site with and increase in accuracy.
Acknowledgement
Dr Neelkamal Kapoor, Professor and Head, Department of Pathology, GMC, Bhopal.
Dr Reeni Malik, Professor, Department of pathology, GMC, Bhopal.
References:
1. Lumley JSP, Chan S, Harris H, Zangana MOM . Physical signs. 18th edition. Oxford: Butterworth-Heinemann, Oxford, 1997. View Review
2. Celeste NP, Williams JF. Fine needle aspiration biopsy of the head and neck. USA: Butterworth Heinemann; 1996. p 1–13.
3. Gamba PG, Messineo A, Antoniello LM, Boccato P, Blandamura S, Cecchetto G, Dall'Igna P, Guglielmi M. A simple exam to screen superficial masses: fine-needle aspiration cytology. Med Pediatr Oncol. 1995 Feb;24(2):97-9.
View Abstract
4. Watkinson JC, Wilson JA, Gaze M, Stell PM, Maran AGD. Stell and Maran’s Head and neck surgery, Butterworth-Heinemann, Oxford, 4th edition, chapter 2; 2000. p 20-21. View Textbook
5. Russel RCG, William NS, Bulstrode CJK. Bailey and Love’s short practice of surgery. 24th edition. London: Arnold; 2004 View Website
6. Afridi S, Malik K, Wahed I. Role of fine needle aspiration biopsy and cytology in breast lumps. J college of Physicians and Surgeons Pakistan. 1995; 5:75-7.
7. Burnand KG, Young AE, Lucas J, Rolands BJ, Scholefield J. The new Aird’s companion in surgical studies. 3rd edition. China: Elsevier; 2005. View Website
8. Howlett DC, Harper B, Quante M, Berresford A, Morley M, Grant J, Ramesar K, Barnes S. Diagnostic adequacy and accuracy of fine needle aspiration cytology in neck lump assessment: results from a regional cancer network over a one year period. J Laryngol Otol. 2007 Jun;121(6):571-9. Epub 2006 Nov 30. View Abstract
9. Schwarz R, Chan NH, MacFarlane JK. Fine needle aspiration cytology in the evaluation of head and neck masses. Am J Surg. 1990 May;159(5):482-5. View Abstract
10. Edward J, Young MD, et al. Needle aspiration cytologic biopsy in head and neck masses. The American Journal of surgery. 1981 Oct;142(4).
11. Tilak V, Dhaded AV, Jain R. Fine needle aspiration cytology of head and neck masses. Indian J Pathol Microbiol. 2002 Jan;45(1):23-9. View Abstract
12. Ahmed T, Naeem M, Ahmad S, Samad A, Nasir A, et al. Fine needle aspiration cytology (FNAC) and neck swellings in the surgical outpatient. J. Ayub Medical College Abbottabad. 2008; 20(3):30-32 View Article